|
|
|
 |

|
|
A Flawed History of Radiation Protection
by John Cameron, Ph.D.
The Angry Genie: One Man’s Walk through the Nuclear Age
Karl Z. Morgan and Ken M. Peterson
Norman, Okla.: University of Oklahoma Press, 1999
Hardcover, 240 pp., $24.95
(Reprinted in full from from Summer 2000 issue)
|
|

K.Z. Morgan (1907-1999) was one of a small handful of pioneers in radiation protection. At some point midway in his career, for reasons not made clear in his biography, he became radiation-phobic. (Oak Ridge National Laboratory)
|
Dr. K.Z. Morgan, the subject and principal author of this biography, was a respected radiation protection scientist (health physicist), who died at age 92, shortly after this book was published. If his silent co-author had been a health physicist, instead of “one of the best trial lawyers in America,” as the book jacket proclaims, the book would have had fewer errors.
The preface indicates that the second author, Ken Peterson, served as editor of the book and contributed most of two chapters, which are not identified. The book is largely autobiographical, and reads as though it came from the pen of Dr. Morgan. This review is written, therefore, as though Morgan is the only author.
K.Z. Morgan (1907-1999) was one of a small handful of pioneers in radiation protection, beginning with the Manhattan Project during World War II. As a leader in the field of radiation protection, he founded the Health Physics Society in 1955, and the Health Physics journal in 1958. He was also the first president of the International Radiation Protection Association (IRPA) in 1966. For these contributions to the field of health physics, he should be honored. At some point in his career, however, Morgan turned to radiation phobia.
Scare Tactics
My main concern with this book is its apparent attempt to frighten the reader with large numbers about radiation danger. The author makes no effort to help the reader understand radiation, such as by expressing radiation in terms of Background Equivalent Radiation Time (BERT),1 which would enable people to understand how minuscule a radiation dose comes from medical X-rays, for example, compared to the natural radiation one receives by living at a high-elevation.
An example of the use of big numbers to scare people appears on page 140, where Morgan quotes from the testimony of radiophobe Dr. John Gofman in the Kerr-McGee/Karen Silkwood legal case. Gofman was giving testimony about the dangers of 1 nanocurie of plutonium in the body: “Two thousand times a minute these bullets, alpha particles are coming out . . . . delivering 5 million of those volts of energy, each one. So, it’s a fantastic projectile. The alpha particles in the lungs, it is hitting right through the cells of the lung with 2.5 million times more energy that you would get from a carbon burning. So you see, expecting that your cells are not going to be damaged by that would be the about the same expectation when somebody might talk to you and say ‘Well, a small amount of this won’t hurt you.’ That is such an absurd nonsense notion that one wonders how anybody could think of it.”
The reader is never told that our cells are being continuously bombarded by high-energy alpha particles in the lungs, and by beta and gamma rays from natural radioactivity throughout our body. There are more than a half-million such projectiles each minute in a 150-pound human being. Billions of our cells are hit each day, and in a year, essentially every cell in our body has been hit. Yet, cancer is a comparatively rare disease, except in the aged. If cancer were completely curable, the average lifespan would only increase by three years.
In regard to alpha particles, which Gofman considers so dangerous, it has long been known that most of our background radiation is from the alpha-particle dose to the lungs from radon progeny. If this alpha radiation were a significant cause of lung cancer, we would expect the states with the highest radon levels to have the most lung cancer. The opposite is the case.
A study of lung cancer in three mountain states with radon levels five times higher than in three Gulf States showed that the lung cancer death rate was 40 percent lower in the mountain states.2 Similar data were published by B.L. Cohen in 1995.3
Also, Morgan does not mention that cigarette smokers have much higher lung doses from the alpha emitters on the smoke they pull into their lungs. The dose to the lungs of smokers is estimated to be 8,000 to 16,000 millirem in a year. This is far greater than the lifetime dose of most radiation workers. It should also be compared to the effective annual dose to the body from all background radiation, including radon progeny, of only 300 millirem. One wonders why cigarette packages have never had a warning about their radioactivity.
The preface indicates that the book is intended for the general public, “but also as a challenge to those who are, or seek to be, health physicists.” If it is indeed a “challenge” to health physicists, it is inappropriate for the general public. Most health physicists have a background with which to evaluate the exaggerated risk statements in this book. Most of the public will not.
The public is generally unaware that most radiation scientists do not believe that there is any risk from low-level radiation. They are also unaware that there is no evidence that even high levels of background radiation can cause cancer, and that, in fact, there is evidence that high levels of natural radiation stimulate the immune system.4
|
|
|
|
|
|

Oak Ridge workers around 1950, at the time Morgan worked at the lab, are here being checked for radiation contamination. The individual at left is checking himself with a hand and foot monitor, while the other worker is being frisked by a health physics technician. (Oak Ridge National Laboratory)
|
‘Disappointment and Anger’
The “genie” in the title refers to the release of nuclear power in the first atomic bomb test in July 1945, and is mentioned only a few times in the text. The “angry” part of the title, as the reader will become aware, is Morgan himself, who is angry for being ignored by the profession he founded. One can sympathize with him, but that does not mean one has to agree with him.
The anti-nuclear community will welcome this book, written by a distinguished scientist whose dominant theme is the great risk from ionizing radiation. For example, in discussing “unsafe” features of nuclear power reactors, Morgan writes in the Preface:
“I am left with a sense of disappointment and anger. The once proud profession of health physics that I helped create over fifty years ago and that was infused with high professional and scientific stature has sunk to a new low.” Later, in chapter 7, “The Advance and Decline of Health Physics” he writes:
“For the past twenty years , health physics, in its mission to protect and defend persons receiving radiation exposures, has sometimes fallen flat on its face. . . . I am convinced that health physics in recent decades has sacrificed its integrity. Certainly there remain some true professionals who will not shade the truth to appease their employers, but they are in the minority.”
Many health physicists will read this book with interest because of its history of the early days of health physics, and they will appreciate the contributions of the author. But they will disagree with the author’s index listing, “Health physics, careless scientists.”
The author further demeans the field that he pioneered, by predicting many radiation deaths, although the book describes only a few actual deaths from radiation. In fact, as the book does not chronicle, medical and industrial uses of radiation and radioactivity have been exceptionally safe. Radiation accidents are so rare, in fact, that they receive a disproportionate amount of publicity when they do occur. For example, the minor criticality accident in Japan, Sept. 30, 1999, resulted, eventually, in 2 deaths, but the day after the accident, news about it occupied 44 percent of the front page of The New York Times. The next day, a commuter train accident in London resulted in 15 deaths, but was given only 13 percent of the Times front page.
Promoting Radiation Phobia
In addition to being disappointed with the health physics profession, Morgan is critical of the two major radiation protection organizations, which publish guidance in the field: the International Commission on Radiological Protection (ICRP) and the U.S. National Council for Radiation Protection and Measurement (NCRP). He was a member of both organizations for 21 years, from 1950 to 1971.
On page 117, Morgan writes, “Like the NCRP, the ICRP is not free of the grip of the nuclear industry.” Apparently, Morgan would want the nuclear industry (and even the medical profession) to encourage the ICRP and NCRP to adopt the policy that even the smallest amount of radiation can cause cancer. I consider this assumption to be basically unscientific and contrary to the interests of the public, the nuclear industry, and the medical profession. Such a wrong belief—that the smallest amount of radiation causes cancer—is a major cause of radiation phobia in the world.
This reviewer is not happy with the ICRP and NCRP for a different reason: The pronouncements of these organizations are partly to blame for the present worldwide radiation phobia. In 1977, the ICRP adopted the assumption that risk from ionizing radiation is proportional to the dose, down to zero dose, in order to simplify radiation protection administration. This assumption, known as the linear no-threshold (LNT) model of radiation risk, has become accepted as dogma, despite contradictory data now, and at the time it was adopted by the ICRP. Various other national radiation protection bodies, including the NCRP, followed suit and adopted the LNT model.
Both groups, IRCP and NCRP, are private organizations, which are not subject to overview by any other body. They select their own members, who tend to agree with their stated positions. Their financial support comes from research contracts and thus does not always represent the public’s interest. For example, they have made few recommendations to reduce unnecessary radiation from medical X-rays, the largest human-made source of radiation to the public.
From Threshold to No-Threshold
In 1943, when Dr. Morgan entered the field of radiation protection, he believed the then-accepted philosophy that radiation, like other toxic substances, was safe up to some threshold dose; this is called the threshold model of risk. Morgan does not explain why he reversed this view, and became a firm believer in the LNT model.
In chapter 2, in a section titled “Research at ORNL: Our Mistaken Belief in a Threshold Hypothesis,” one might expect him to explain why he became a believer in the LNT assumption. He does not. Instead, he describes some of his research at Oak Ridge National Laboratory, and states merely, “Early on we all accepted the threshold hypothesis.”
He then discusses his human radiation experiment, and he describes two instances of carelessness by the ORNL staff, but he gives no information related to the title of the section. Perhaps, at 91, when the book was completed, his mind drifted off.
There is a good reason why Morgan could give no evidence to support the LNT model of risk; it is theoretically impossible to do so! Even the Japanese atomic bomb survivors had a threshold for the induction of leukemia of about 0.25 Gy, a dose roughly equal to 100 years’ accumulation of background radiation.
Genetic Effects
The area Morgan is most concerned with is the genetic effects of radiation. Certainly, fruit flies demonstrate radiation-induced mutations. However, fruit flies do not have the advantage of the p53 gene. In human beings and other higher animals, the p53 gene signals damaged cells to die. A study of the 90,000 children and grandchildren of atomic bomb survivors in Japan found no increase in mutations. The genetic effects of low-level radiation are not a problem for society. .
Morgan also mentions the health risk to radium dial painters early in the 20th century. These workers accidentally ate small amounts of radium as they touched the paint brush to their mouth, to give it a sharper point. He does not mention, however, that radium dial painters did not develop bone cancer from radium unless they had a very high skeletal dose—greater than 10 Gy (200 Sv). That is 10,000 times greater than the present recommended annual dose limit for radiation workers! Above that threshold, the dial painters had an incidence of bone cancer of about 28 percent, independent of the dose.5
Perhaps more remarkable is the finding that no dial painters who started work after 1925 developed bone cancer. That was the year the radium dial industry forbade the workers to touch the brush to their mouths.
|
|
|
|
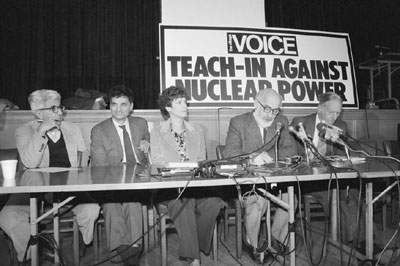
Morgan’s co-thinker, Dr. John Gofman (second from right), speaking at a Teach-in Against Nuclear Power at New York’s Riverside Church in May 1979. With him on the podium are Barry Commoner (left) and Ralph Nader (second from left). (Bettmann/Corbis)
|
|
|
|
|
Human Radiation Experimentation
The reader may be upset by the author’s description of human radiation experimentation. Morgan recounts an incident about his colleague, Dr. Robert S. Stone, the associate director of health of the Manhattan Project who had an office next to his in Tennessee. Morgan writes:
“Health physics owes a debt to Robert S. Stone. ... Stone insisted that we implement a conservative approach in determining accepted levels of exposure and accumulated radiation dose.” In the spring of 1945, Stone entered Morgan’s office and said, “Karl, you remember that black truck driver who had multiple fractures in an accident and we rushed him to the [military] hospital? ... Almost all of his bones were broken and we were surprised that he was still alive when he got to the hospital, we did not expect him to be alive the next morning so this was a good opportunity we’ve been waiting for. We gave him large doses by injection of plutonium-239. We were anticipating collecting not just urine and feces but a number of tissues, such as the skeleton, liver, and other organs. This morning when the nurse went into his room, he was gone. We have no idea what happened, where he is, but we’ve lost valuable data we were expected to get.”
Morgan writes a little later, “I heard nothing more about this until years later, when I saw in the Knoxville paper a death notice for the black truck driver, whose name I remembered.”
It would appear that little effort was made to locate the missing “terminal” patient loaded with plutonium. My guess is that, the plutonium did not contribute to his death.
The author describes other examples of inappropriate and unethical studies using radiation and radioactivity. These ethical problems were not caused by the fictitious “angry genie,” but by the faulty judgment of human beings who did the research.
A Question of Dose
Throughout, the author fails to discuss the importance of the dose in judging the ethics of radiation research on human beings. Medical science progresses by research. The only way to evaluate a new medical modality is to do research on human subjects. In such cases, it is the size of the dose that determines if there is a health risk. I doubt that more than a few human experiments described in this book shortened the life of the subjects. However, independent of the dose question, the subject always has a right to know if she or he is participating in a medical experiment.
In the 1940s, the attitude of medical doctors toward using patients for research was very different than it is today.
|
|
|
|
|
|
|
Putting Radiation in Perspective
In my bone research, in the 1960s, I exposed hundreds of human beings to ionizing radiation, including myself and my two daughters. The amounts of radiation were trivial. Our daughters received a hundred times more radiation while camping a few days in Glacier National Park.
I had invented the first accurate instrument (bone densitometer) in 1960 for measuring the amount of bone in the living body. There are now about 25,000 such instruments in the world used for diagnosing and evaluating osteoporosis.
The original instrument used a narrow beam of monoenergetic photons from lead-210, a natural radioisotope of lead, which was produced from old radon seeds. During the measurement, we moved the narrow beam across the forearm and measured the amount of radiation that came out the other side. The mass of bone can be accurately calculated from the reduction of beam, as a result of its absorption in bone.
The radiation dose to the subjects was roughly equal to the dose they receive from nature in a few hours—less than 1 percent of the exposure from an X-ray of the arm. These experiments on human beings were needed to determine the normal range of bone mass as a function of age and sex. The research was approved by the human-use committee of the University of Wisconsin Medical School.
All subjects (or their parent) had to sign a form saying they understood the risk and giving permission for the study. I have not the slightest feelings of guilt about these human radiation studies. —John Cameron
|
|
|
|
|
|
|
The Atomic Bomb Blunder
The author puts a sad twist on the history of the dropping of the atomic bomb on Hiroshima. Morgan writes: “Atomic power was used needlessly, I believe, and in revenge—to take the lives of hundreds of thousands of Japanese men, women, and children.” He continues this theme in Chapter 2, “The Truman Administration’s Greatest Mistake,” where he writes “... I remain firmly convinced that President Harry S. Truman and Major General Leslie R. Groves blundered in their decision to order atomic bombs to be dropped on Hiroshima and Nagasaki.”
Later, Morgan makes it clear that: “Both Byrnes [Secretary of State] and Stimson [Secretary of War] strongly favored bombing without warning. ... Truman’s personal journal contains evidence that he favored a warning.” The author suggests that the second atomic bomb, which used plutonium rather than enriched uranium-235, was deployed because “the U.S. military saw Nagasaki as an opportunity to determine how the plutonium weapon rivaled the uranium device.”
Perhaps the most disastrous effect of the bomb on society was to produce the huge amount of radiation phobia today, which hampers the use of nuclear power and the medical uses of radiation. Most of the initial atomic bomb victims died from heat and blast, the same as they would have from conventional bombs. The number of deaths from radiation was considerably smaller. The total deaths from the two atomic bombs was between 100,000 and 200,000—about the same number of casualties there were when the United States fire-bombed the center of Tokyo a few months earlier, leaving a million people homeless.
Most Americans don’t remember this, but the Japanese do. I don’t see a great difference in the ethics of fire bombing the center of Tokyo or the dropping of the atomic bombs. Both are wrong.
More Exaggeration
Morgan exaggerates the final number of fatalities from the atomic bombs. He writes: “If one adds the latent deaths from these two bombs, the total number of Japanese killed reaches a half a million.” The author fails to mention that more than 50 years after the atomic bombs were dropped, the total number of deaths from radiation-induced cancer is only about 400—an average of less than 10 deaths a year among the roughly 100,000 atomic bomb survivors.
An even more important statistic is that the atomic bomb survivors are living longer on the average (even including these cancer deaths) than similar Japanese who were not exposed to the atomic bomb radiation. The large number of latent deaths are a fiction. Similar examples of exaggeration occur throughout the book.
On the positive side, Morgan gives a very reasonable recommendation for storing used nuclear fuel (nuclear waste). He writes (p. 157): “The best move for the present time is to let the fuel assemblies cool in the power reactor ‘swimming pools’ for at least three years to permit radioactive decay of some of the short-lived fission products and then ship them to a temporary and retrievable storage facility. Then it would be up to a future society to determine the best next step. It is my hope that 50 or 100 years from now, society will have advanced and will have arrived at the best long-term solution.”
Such a procedure is already in use by Northern States Power for its nuclear power plant in Minnesota. The old fuel is stored in “dry cask storage”—sealed in large double walled stainless steel containers on site. These are easily monitored and offer no risk to the public. The State of Minnesota limits radiation to the public from dry cask storage each year to 0.05 millirem—much less radiation than they receive from nature in a day or from one jet flight.
Overall, an Unbalanced View
In summary, this book has a large amount of interesting historical information on radiation problems relating to the atomic bomb project, However, it greatly exaggerates radiation risk, which will only increase the anxiety of many readers, and may even scare some patients away from having a needed mammogram or other radiation study. The theoretical or latent radiation deaths predicted by the authors can never be found. Studies of U.K. radiologists—the occupational group that receives the most occupational radiation—show a reduced cancer death rate compared to other medical specialists.
The public deserves a book that gives a more accurate picture of the benefits of radiation.
John Cameron is a Professor Emeritus at the University of Wisconsin at Madison and a Visiting Professor at the University of Florida. An internationally known radiation scientist, he is considered one of the world’s pioneers in medical applications of physics. In the 1960s, he developed thermoluminescent dosimetry, the basic method for measuring radiation received by nuclear workers.
|
|
|
|
|
|
Notes
1. See the author’s article, “A New Radiation Unit for the Public,” 21st Century, Spring 1998, p. 5. See also, “Are X-rays Safe?” on the Internet: http://www.medinfo.ufl.edu/other/cameron/rads.html)
2. J. Jagger, 1998. “Natural Background Radiation and Cancer Death in Rocky Mountain States and Gulf Coast States,” Health Physics (Oct.), pp. 428-430.
3. B. L. Cohen, 1995. “Test of the LNT Theory of Radiation Carcinogenesis in the Low-Dose, Low-Dose-Rate Region, Health Physics, Vol. 68, pp. 157-174.
4. L.E. Feinendegen, V.P. Bond, and C.A. Sondhaus, 1998. “Low-level Radiation May Protect Against Cancer,” Physics and Society News (April).
5. R.D. Evans, 1974. “Radium in Man,” Health Physics (Nov.), pp. 495-510.
6. P.G. Smith and R. Doll, 1981. “Mortality from Cancer of All Causes Among UK Radiologists,” British Journal of Radiology (March).
|
|
|
|
|
|
|
|