|
|
|
 |
|
|
|
|
|
Problems of U.S. Policy On Radiation Protection
by Zbigniew Jaworowski, M.D., Ph.D., D.Sc. and Michael P.R. Waligórski
Two eminent radiation experts, discuss the deliberate misrepresentations, omissions, and bias in a report by the U.S. National Council on Radiation Protection, at the expense of the general welfare.
|
|
For More on Low-Level Radiation:
• The Truth About Chernobyl Is ToldI (Winter 2000-2001)
•It’s Time to Tell the Truth About the Health Benefits
of Radiation (Summer 2000)
• A Flawed History of Radiation Protection (Summer 2000)
|
|
|
|
|
Zbigniew Jaworowski, M.D., Ph.D., D.Sc., is at the Central Laboratory for Radiological Protection, Warsaw. His studies include the internal contamination of man and animals with radionuclides, the development of analytical methods for detection of pollutants in the human body and environment, the metabolism of radionuclides, and the biological effects of ionizing radiation. He was the principal investigator of three research projects of the U.S. Environmental Protection Agency involving pollutants in the global atmosphere, and he has organized ten expeditions to polar and high-altitude temperate glaciers to measure, for the first time, the mass of stable heavy metals and the activity of natural radionuclides entering the global atmosphere from natural and man-made sources. He has written 270 scientific papers, 4 books, and 100 articles for popular audiences.
Michael P.R. Waligórski, Ph.D., is head of the Medical Physics Department, Center of Oncology, in Krakow, Poland. He has been a professor and researcher at many universities internationally, including the University of Nebraska at Lincoln and Brookhaven National Laboratory in the United States. His research areas include nuclear radiation and medical physics, radiobiology, radiotherapy, and radiation protection. He has authored more than 150 publications and several textbook chapters.
|
|
|

Impartiality Forgotten
Skewing the Issue of DNA Damage
Thyroid Cancers and Chernobyl
Other Omissions
Arbitrary Definitions
The Fraud of the ‘Healthy Worker’ Effect
Chronic vs. Fractionated Exposure
More Bias
Failing the Reality Test
References
|
|
The National Council on Radiation Protection and Measurements (NCRP) has a long history of concern over the effects of ionizing radiation. Chartered by the U.S. Congress as a nonprofit corporation in 1964, it contributed a great deal to establishing radiation protection criteria and systems in the United States and worldwide. However, in its recent report (No. 136), “Evaluation of the Linear No-Threshold Response Model for Ionizing Radiation” (NCRP 2001), the high scientific standards and impartiality of the NCRP have melted into thin air, sacrificed to defend an obsolete and untenable linearity paradigm. This unfortunate NCRP policy is discussed and criticized here.
The report is 287 pages long, and our criticism could be as bulky. However, we shall limit ourselves to comments that demonstrate the unscientific nature of this report. The subject of NCRP-136-namely, that there is a linear relationship between radiation dose and biological effects-is a central issue in the global radiological protection system. Adherence to this assumption is why current radiation regulations are excessively complicated, and its scientific and pragmatic principles in disarray. The consequences of this assumption lead to what the former president and honorary member of the NCRP, Lauriston S. Taylor, defined as “deeply immoral uses of our scientific heritage” (Taylor 1980).
Since its inception, the NCRP has been wedded to the philosophy that even the lowest, near-zero, radiation exposure may carry some risk. (See, for example, the NCRP 1949 report, which was published in 1954-NCRP 1954.) Today, this concept is called LNT, the linear no-threshold assumption.
This oversimplified LNT approach was based on early results of radiogenetic experiments with insects and mice, which did not take into account the human body’s repair processes. Also, in the early years, there was a practical necessity of protecting a relatively small group of workers in a rapidly developing nuclear industry. Over the years, however, we learned that no radiogenetic disturbances were ever found in man, not even among the progeny of Hiroshima and Nagasaki victims, and that radiogenic cancer does not result from direct radiation damage to a single DNA strand (UNSCEAR 2000).
When applied to the protection of the public, both locally and internationally, LNT has had far-reaching negative consequences, including the rejection of nuclear energy based on fear, the enormous costs involved in implementing unnecessarily restrictive rules of protection, and paranoiac mass radiophobia, such as we have seen after the Chernobyl incident. All of these consequences involve ethical issues (Jaworowski 1999). Each human life hypothetically saved in the United States by implementation of the present radiation protection regulations is estimated to cost about $2.5 billion. Such costs are absurd and immoral. Billions of dollars are spent year after year for the imaginary protection of human beings from radiation, while there is a scandalous lack of much smaller resources for real life saving in poor countries.
Impartiality Forgotten
In the past, the NCRP has endeavored in its reports to present various aspects of the LNT assumption, as well as the evidence refuting it and questioning its scientific legitimacy (see, for example, NCRP 1975). This impartial approach, although laudable, was only cosmetic. In fact, the NCRP always proposed the LNT as the basis of radiation protection, including its logical consequences, the principle of collective dose, and the radiation “as low as reasonably achievable” slogan (later renamed ALARA).
The ALARA slogan had a terrifying impact on public opinion. People became convinced that ionizing radiation was extremely dangerous and should be avoided by all means, at any cost, and at any level, even if it were near zero. But in the most recent NCRP Report, No. 136, even this makeshift impartiality was forgotten.
The authors of the report do not try to objectively present the scientific evidence for and against the validity of the LNT, but instead merely propagate the LNT by errors of omission and commission. Two methods were used throughout the report. First, the material was selected so that the many important papers contradicting LNT were not presented at all. Second, pro-LNT publications were presented in great detail, while the report merely provided references to a few papers that disagree with these publications, without presenting the data or arguments of the critical papers.
The report concentrates almost exclusively on the detrimental effects of radiation, downplays radiation’s beneficial effects, and does not mention the important studies that suggest that ionizing radiation may be essential for life (for example, Planel et al. 1987).
Skewing the Issue of DNA Damage
The main object of radiological protection of the public is to avoid the risk of cancers and genetic disorders caused by DNA damage. Information on the rate of spontaneous and radiation-induced DNA damage in mammalian cells is essential for any evaluation of this risk. However, the NCRP report does not inform the reader that 70 million spontaneous DNA damages occur per each cell of his body per year, compared to 2 damages per cell per year induced by the current, excessively low, radiation dose limit of 1 mSv [millisievert] (Billen 1990). We can survive this gigantic stream of spontaneous DNA damage only because human organisms are armed with a powerful and efficient defense system. Ionizing radiation contributes an infinitesimally small fraction of this stream of DNA damage.
Double-strand breaks of DNA are more difficult to repair than are single-strand breaks. About 40 spontaneous double-strand breaks occur in each mammalian cell in a year. This is about 1,000 times more breaks than those that occur after a natural background dose of 1 mSv (Stewart 1999). Among all the complex damages induced by ionizing radiation, double-strand breaks constitute only about 20 percent, with other clustered damage constituting some 80 percent.
The clustered damages are regarded as critical lesions, which produce the lethal and mutagenic effects of ionizing radiation (Sutherland et al. 2000). Normal cells are able to repair these damages with fidelity, as recently confirmed by E. Moustacchi (2000). Moustacchi stated that for many genotoxins and agents, very low doses may have no effect at all in normal cells. The papers on this subject by Moustacchi, Stewart, and Sutherland et al., along with many others that are in disagreement with the pro-LNT line, are not cited in the NCRP report. No doubt, these papers were ignored because they show how nonsensical the dose limit of 1 mSv is.
The report features (p. 74) a study on unstable chromosome aberrations in the peripheral blood lymphocytes of 31 Chernobyl cleanup workers, which shows linear dose-response curves (Semov et al. 1994). (In other words, the greater the dose, the greater the aberration.) However, a new, much larger study on 4,833 cleanup workers, with more than a quarter of a million metaphases examined (Littlefield et al. 1996), is not mentioned. The data from Littlefield et al. demonstrate that the frequency of chromosomal aberrations is lower among the exposed workers than among the control group, and that there is no increase in the mean, median, or range in chromosome aberrations in lymphocyte cultures. These results are consistent with the negative results of several studies of cancer incidence in Chernobyl cleanup workers. Ignoring this information attests to the biased style of the NCRP-136 report.
The report states (p. 136) that so-called “ecological” studies in epidemiology “cannot be regarded as trustworthy and should not be relied upon to assess either the presence or absence of excess radiation-induced cancer at low doses.” But this view is applied only if such studies present evidence against LNT; otherwise, the NCRP report accepts such “ecological” studies. For example, the report covers one such study to show that the increase of thyroid cancer registration in Belarus is allegedly the result of Chernobyl fallout, and that it is directly proportional to radiation dose (p. 161).
Most of the post-Chernobyl epidemiological studies reviewed in the NCRP-136 report, in fact, are of the “ecological” type. But, in the case of B.L. Cohen’s studies (1995), showing that high levels of residential radon are associated with lower lung cancer incidence, the report condemns the data as “not trustworthy” (see discussion below). However, when arguing that thyroid cancers are caused by low doses of Chernobyl radiation, this condemnation is forgotten, and the results of these ecological studies are defined as “convincing,” and “conform[ing] reasonably well to the magnitude of dose by region.” (In fact, in these Chernobyl studies there was a lack of reliable personal thyroid dosimetry and the estimates of thyroid doses were highly uncertain, as opposed to the high quality dosimetry in Cohen’s studies.)
Thyroid Cancers and Chernobyl
No in-depth discussion of screening effect, the most probable cause of the increase in Chernobyl thyroid cancer registration, is provided in the report. This topic is extensively documented in the 115-page-thick Scientific Annex J of the UNSCEAR 2000 report, which is well known as the primary scientific assessment of the effects of the Chernobyl accident. As the UNSCEAR 2000 report documents, after this accident, the highest thyroid cancer incidence of 0.027 percent appeared in the Bryansk region of Russia, where the average thyroid dose was 37 mGy [milligray]. The highest incidence in Belarus, 0.018 percent, was found in the Gomel region, where the thyroid dose was 177 mGy); and in the Ukraine, the highest thyroid cancer incidence, 0.005 percent in the Kiev region, occurred where the average thyroid dose was 380 mGy). Thus, incidence of thyroid cancer is by no means directly proportional to dose.
Furthermore, the normal incidence of “occult” thyroid cancers is very high in most countries. Although such cancers do not cause any visible clinical disturbance, they are histologically malignant, aggressive, and the same as the “Chernobyl” cancers. They are usually discovered in the course of a postmortem pathological examination, or by imaging studies. The autopsy prevalence of occult thyroid cancers in various countries ranges from 4.5 percent to 36 percent (Moosa and Mazzaferri, 1997; Tan and Gharib, 1997). The normal incidence of the occult thyroid cancers is about 1,000 times higher than the highest incidence of reported thyroid cancers in post-Soviet countries; thus the potential of the screening effect is enormous, but this is not discussed at all in the report.
The data on increased reporting of thyroid cancers in the NCRP-136 report are limited exclusively to children. However, since the studies of Ivanov et al. in 1996 and 1997, which were reviewed in the UNSCEAR 2000 report, it is well known that the increase in those adults who were screened (such as recovery operation workers) is similar to the increase in children.
The NCRP-136 report states that “the excess of histologically confirmed thyroid cancer has been so large that it cannot be attributed only to increased surveillance.” This statement does not appear to be correct. According to the report, “. . . during 1990 and 1994 a total of 315 thyroid cancers in children were observed in Belarus, which was a 30-fold excess over the numbers observed there in the previous 10 y[ears].” A similar 21-fold excess of thyroid nodules, caused by the screening effect, was observed in the United States between 1974 and 1979 (Ron et al. 1992). One should also note that a similar screening effect was found for chronic lymphocytic leukemia (deemed not to be increased by radiation exposure) among the Russian recovery operation workers (documented in UNSCEAR 2001-unpublished). The screening effect, and the influence of occult thyroid cancers on it, are virtually ignored by the NCRP.
Other Omissions
The NCRP-136 report omits important information from the UNSCEAR 2000 Report: for the 15 years after the Chernobyl accident, there was no increase in the incidence of leukemia or any solid cancers (except thyroid cancer, which, arguably, is a screening effect). The report also neglects to inform the reader that there was a total lack of radiation-induced hereditary disturbances both in the Chernobyl population, and among the progeny of survivors of the World War II atomic attack in Japan. These omissions should serve as a warning of how deeply biased this report is.
The information on an exceptionally high risk of radiation-induced leukemia is presented for the nuclear test code-named SMOKY. In this test, the average dose was only 4.66 mSv and the ratio of observed to expected numbers of leukemia cases was 10.0 to 4.0; that is, the incidence of leukemia increased by a factor of 2.5. However, there are contradictory data from another nuclear test (code-named Operation Greenhouse), where there was an average dose of 13 mSv, and the observed to expected numbers of leukemia cases was 1.0 to 4.4 (which corresponds to a deficit of leukemia cases of 73 percent).
The substantial published evidence and consensus (for example, Robinette 1985 and Doll et al. 1998, and the references therein) that there are no adverse effects to the populations of nuclear weapons observers but rather hormetic (beneficial) ones, was not reflected in the NCRP-136 report.
In a discussion of lung cancers, the report notes an epidemiological study of Canadian tuberculosis patients. This study showed that after irradiation with doses of up to 0.99 Sv [sievert], the patients had a clear deficit of lung cancers. Yet, the NCRP-136 report characterizes this very positive result by stating only that it showed that the risk “was not elevated.”
An even worse treatment was handed out to the excellent study of Tokarskaya et al. (1997) on a unique group of Eastern Urals Mayak nuclear reprocessing plant workers exposed to plutonium, in which smoking was fully accounted for as a confounding factor. The authors of the NCRP-136 state incorrectly (p. 171) that this study “showed an excess of lung cancer down to levels of about 1 Sv.” In fact, an excess of lung cancer incidence was observed by Tokarskaya et al. starting at radiation levels higher by a factor of 20-that is, between 20.1 and 344 Sv. But between 0.81 and 6.0 Sv, a 21 percent decrease in lung cancer incidence was found; and between 6.1 and 20.0 Sv, there was a 28 percent decrease. This important finding suggests the existence of a threshold for radiation effects, below which there are beneficial or hormetic effects. Tokarskaya et al. concluded 1) that the “dose-effect for smoking had a linear character,” and 2) that the “dose-response relationship for plutonium incorporation corresponded to the nonlinear threshold relationship,” with a threshold of about 3.7 kBq [kilobequerel] of plutonium-239 body burden, or 0.8 Gy [gray].
On the same page, the report cites the papers of Hohryakov and Romanov (1994) and of Koshurnikova et al. (1997), as showing “an excess of lung cancer” in workers of the Russian plutonium facility, without informing the reader that a deficit of lung cancers was found at lower doses.
We observe here not simply an incompetent and careless presentation of published data, but also a pattern of concealing important information that strongly refutes the LNT. Unfortunately, this pattern is typical throughout the NCRP-136 report
|
|
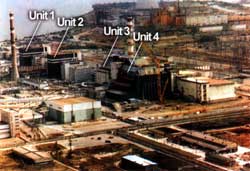
The Chernobyl nuclear reactor in Ukraine. The proliferation of radiophobic hysteria all around the world was the real "disaster."
|
|
The Real Chernobyl Disaster
The LNT assumption, as implemented by national regulations and official policy, was the prime cause of the disastrous consequences of the 1986 Chernobyl accident. Enormous loss of resources, the invention of the status of a “Chernobyl victim,” awarding costly social privileges to large groups of such “victims,” unnecessary relocation and pauperization of hundreds of thousands of persons, and epidemics of psychosomatic diseases throughout vast territories of the former Soviet Union, were not caused by radiation, but followed from the adherence to the LNT-based recommendations of the international radiation protection organizations. Notable among these are the International Commission on Radiation Protection and the International Atomic Energy Agency.
This is one of the most important lessons learned from the Chernobyl catastrophe, which should be taken into account in the current plans to counter nuclear and radiation terrorist attacks. Decades of promoting the LNT-based radiophobia have made the societies of developed countries extremely vulnerable to the psychological consequences of such activities. One of the consequences of NCRP Report 136 will surely be the perpetuation of mass radiophobia.
|
|
|
|
Arbitrary Definitions
In its definition of “stochastic [probabilistic] effects,” the NCRP-136 authors have an arbitrary premise of a “no threshold” response and linearity. The report differentiates between “stochastic” effects-the severity of which allegedly does not vary with dose, and “deterministic” effects-the severity of which increases with dose. Yet, this is an empty and obsolete definition in view of current information on the mechanisms of carcinogenesis and genetics. Medicine does not recognize such a distinction, which was introduced in the early 1970s by the pro-LNT lobby in radiation protection.
The lack of dose-related severity in stochastic effects, trumped up as the main difference between them and deterministic effects, is not true. As demonstrated by radiation scientist Walinder (1995), many radiogenic cancers in man and in experimental animals show greater histologic and clinical malignancy after high radiation doses, than after smaller ones. Also, the latency time is shortened when the dose increases, so that malignant tumors can be more “severe” because they have had time to develop during a lifetime. This was acknowledged by the NCRP in its 1975 publication.
The notion of “stochastic” and “deterministic” effects is a tacit introduction of the LNT thinking template into radiation protection, which occurred in the late 1970s. These two words replace the clear, simple, and informative terms used for decades, such as “somatic” and “genetic,” early and late effects, neoplasmatic and hereditary diseases, and so on. Except for selling the non-threshold ideology, these two newer terms-stochastic and deterministic effects-carry no useful information.
Low radiation doses are well known and documented to cause life-span increases. Yet, in the chapter on “Life Shortening,” the NCRP reports from a study by Walburg (1975), that in experimental animals the “shortening of life span by low-to-intermediate doses of whole-body radiation has been observed to result primarily from increased or accelerated rates of neoplasia.” However, it fails to cite the same author when he reports that “when only non-neoplastic causes of death were considered, there was no significant effect on life shortening, and the mean age at death increased in irradiated animals relative to controls.”
The NCRP does not report that improved immunity after low-dose irradiation increases the life-span, and no mention is made of the fact that “aging” is not an effect of low doses. In a detailed presentation based on a few papers showing that life-shortening results from neoplastic causes, the NCRP report cites 16 papers that failed to show life shortening at low doses in experimental animals, but does not present their results. Instead, the report characterizes them only as “ostensibly at variance” with the linear increase of life shortening with dose. The report did not present the important study on the effect of chronic irradiation on human embryo cells, at a dose rate corresponding to about 3.65 Gy per year, in which the life-span of cells was longer than of non-irradiated cells (Suzuki et al. 1992).
It is interesting that the radiation effects to the immune system are not discussed at all in the report. The term “immune” is not even indexed, and the classic literature on this issue is not mentioned-for example, Liu et al. 1987 and Makinodan and James 1990-probably because it strongly suggests the existence of hormetic effects, which are in direct opposition to LNT assumption.
In line with this selective approach, the NCRP report does not present the beneficial effects of whole- or half-body fractionated irradiation of patients with tumors to a total dose of about 1.5 Gy, 90 percent of whom showed complete or partial remission (UNSCEAR 1994).
The Fraud of the ‘Healthy Worker’ Effect
The NCRP report states that the so-called “healthy worker effect” is ubiquitous in occupational studies. (This is the alleged self-selection of healthy workers in nuclear-related professions.) But this effect was specifically excluded in the Smith and Doll (1981) study on British radiologists, for which the control subjects were other medical practitioners. One cannot suppose that radiologists were self-selected for initial or later good health in a different way from other medical practitioners.
In a large study of U.S. nuclear shipyard workers (Matanoski 1991), the “healthy worker effect” was explicitly excluded. This study of 30,000 shipyard workers showed a strong hormetic effect of the low radiation doses for lymphatic and haemopoietic cancers and for other effects. The NCRP report chose to disqualify this study on the false ground that it was caused by the “healthy worker effect.” However, as stated in the UNSCEAR 1994 report, this statistically significant decrease in mortality ratio in shipyard workers cannot be caused by the healthy worker effect.
Nevertheless, the NCRP report makes the wholly unfounded statement that “a difference for total mortality, and not just for radiosensitive cancers, supports the interpretation that [worker] selection factors were operative.” However, this effect indicates only that enhanced immunity induced by low radiation doses had a general character, and was active not only for cancers but also reduced infections, inflammations, and many other ailments, as is well documented in the medical literature and in in vivo animal studies.
To take another example: In a study of British radiologists from 1936-54, there was a 39 percent deficit of cancer deaths. If, however, the induction of radiogenic cancers were really a “stochastic” phenomenon (as postulated in the NCRP report), depending simply on the statistical probability of radiation damage in DNA, then the stochastic chance of cancer should be the same for a “healthy” and a “less healthy” worker. The ambiguous concepts of “stochasticity” and “healthy worker effect” are thus in conflict.
No mention is made in the NCRP report that from both these cited occupational studies it is apparent that low doses of radiation are beneficial for the workers. In nuclear shipyard workers, the nuclear workers had 19-24 percent (depending on the radiation dose category) less mortality as the result of all causes, and 9 to 58 percent less leukemia mortality than did the shipyard’s non-nuclear workers. Why, then, after presenting the leukemia data for workers from U.S. nuclear shipyards, does the NCRP report state: “No excess of leukemia was observed”?
The NCRP-136 report cites also the Smith and Doll study (1981) as having “reported excess of total cancers” among the British radiologists. In fact, this paper shows a 39 percent deficit of deaths resulting from all neoplasms for the period 1936-1954, and 21 percent deficit for the period 1921-1954. New data, not cited in NCRP-136, on British radiologists for the period 1955-1979, show a 27 percent deficit of all cancer deaths, and a 37 percent deficit for mortality resulting from all non-cancer diseases (Berrington et al. 2001).
Chronic vs. Fractionated Exposure
The NCRP report fails to express even so much as a reservation about whether health effects in atomic bomb survivors in Japan are relevant to estimating the risk of chronic or highly fractionated exposures in other cases. It uses the high-dose Japanese epidemiological data as a yardstick good for every occasion. However, the lifetime exposures from Chernobyl fallout or fractionated occupational exposures during a few decades, differ from exposures in Hiroshima and Nagasaki by a factor of 1015 (a thousand trillion) in the dose rates.
The biological responses to essentially “instantaneous” high doses from mixed gamma-neutron radiation emitted after nuclear explosions, cannot be a sound foundation to assess the health effects of protracted low-level irradiation, which is typical for the realm of radiation protection and natural background.
The epidemiological data on the Techa River population in the Eastern Urals, contaminated by emissions from military reprocessing plant in Mayak, are presented to show “a statistically significant exposure-response (LNT) relationship” (Kossenko and Degteva 1994). However, the report does not cite a study on the Techa River population from the very same issue of The Science of the Total Environment by Kostyuchenko and Krestinina (1994) showing a statistically significant decrease of tumor-related mortality ranging from 28 percent to 39 percent for dose categories of less than 500 mSv. This is an example of the report’s distorted and biased selection of published information.
Below a dose of 100 mSv, the causal link between radiation exposure and the increase of cancer is entirely speculative (in other words, it doesn’t exist), whereas the statistically significant epidemiological data from numerous studies on occupational, natural, and accidental exposure strongly suggest the decrease of neoplasms. The discussion of the latter evidence in the report’s chapter on hormesis is limited to merely two papers, selected from the several hundred references, abstracts, and summary data provided by the organization Radiation, Science, and Health to which the report refers (Muckerheide et al. 1998).
Furthermore, the report does not present in this chapter a generalized view and theory of hormesis-for example, that of Calabrese et al. (1999). Hormesis, or the beneficial effects of low doses of any noxious agent, is a phenomenon observed for virtually all kinds of chemical and physical agents, and is well known in pharmacology, toxicology, and general medicine. It is a pity that at least part of many hundred papers reviewed recently in 26 reviews published in Calabrese and Balwin (2001) were not discussed in the report. But how could they be, as most of them demonstrate that the LNT is an obsolete concept?
The aim of the NCRP report was to evaluate the applicability of the LNT in the context of radiation protection policies and regulations, which is limited to the effects of low doses, up to about 500 mSv. Why then, in a figure on p. 146, does the NCRP report present the data on leukemia mortality as the result of high doses (up to 4,500 mSv) in Japanese atomic-bomb survivors, while it virtually conceals the data for doses below 0.5 Sv? [See Figure 1.]
Why, in the same figure [Figure 1(b)], at the x-axis representing radiation dose, does the report allow only 3 millimeters for the most important dose category of 1 to 200 mSv, compared to 73 millimeters for the largely irrelevant doses of 500 to 5,000 mSv? By this manipulation, the report conceals the apparent threshold, and the deficit of leukemia below 200 mSv, which is clearly seen in original publication of the cited sources (Shimizu et al. 1992 and UNSCEAR 1994).
The famous paper by Miller et al., on breast cancer mortality in Canadian tuberculosis patients (1989), is discussed in the NCRP report. This paper shows a 27 percent deficit of breast cancer in women in the 0.10 to 0.19 Gy dose category, as compared with the 0 to 0.09 Gy category. This deficit was not noticed by Miller et al. These authors interpreted their results, according to the LNT paradigm, as a straight line from high doses, even though the line falls many standard deviations outside the data points at lower doses. In the NCRP-136 report this deficit of breast cancer mortality in patients from the years 1930 through 1952, is downplayed as “a statistical anomaly.” This was done on the grounds that an update of this study by Howe and McLaughlin in 1995 “lumped” all of the low-dose data into a single data point, to eliminate the possibility of demonstrating the reduced breast cancer in these women!
|
|
|
|
|
|
|
|
|
More Bias
The chapter on Ecologic Studies is exceptionally biased, presenting the arguments of only one side. The discussion is centered on the 1995 study of Cohen, which demonstrated that the LNT predictions of lung cancer mortality caused by residential radon are not confirmed by the highly statistically significant results of the epidemiological study of large populations that are exposed to moderately large variations in radon. Cohen’s results, covering more than 90 percent of the population of the United States, demonstrate that people living in houses with high radon concentration in the air have a lower incidence of lung cancers than those who live in houses with low radon concentration. From among many papers by Professor Cohen on this subject from 1987 to 2000, the NCRP report cites only one.
On the other hand, the report cites many papers to support a statement that ecological studies, such as those performed by Cohen, are intrinsically biased. Cohen has refuted the arguments in these papers, through rigorous scientific analysis in his numerous publications. Yet, none of these publications by Cohen is even mentioned. Cited extensively is a paper by Lubin (1998)-which criticizes Cohen’s work of 1995, using general rhetoric about “the kinds of errors that could affect an ecologic study.” However, Cohen’s reply to the Lubin criticisms, published in the same issue of Health Physics magazine (pp. 18-23) in which the Lubin article appears, is not even mentioned in the NCRP report. In his reply, Cohen analyzed the actual data to show that the so-called “Lubin’s effect” contributes very little to the huge discrepancy between Cohen’s rigorous results and the LNT predictions, and does not offer a plausible explanation of this discrepancy.
Cohen’s work is the largest existing radon study, producing the best statistics ever compiled, and carefully accounting for 54 confounding socioeconomic factors, including smoking. The NCRP’s unfounded discrimination against such an excellent scientific study, because it does not happen to fit the LNT model, is not something the NCRP can be proud of. The report also ignores other studies that consistently confirm Cohen’s results, such as Bogen (1998) or Rossi and Zaider (1997). On the other hand, nine papers of Cohen’s principal opponent, Dr. J.H. Lubin, are in the report’s list of references. In none of these papers does Lubin present convincing arguments that might support the presumption that ecological studies produce erroneous results.
The results of Cohen’s 1995 study, which directly contradict the LNT “predictions,” were statistically much more robust than results of any other study on the relation between lung cancer and residential radon, and the study meets the most rigorous methodological criteria. For example, the graph plotted of this relationship, as found by Cohen, is inconsistent with the LNT predictions of BEIR IV by more than 20 standard deviations. (BEIR IV is the National Academy of Science/National Research Council’s 1988 report by the Committee on the Biological Effects of Ionizing Radiation, titled “Health Risks of Radon and Other Internally Deposited Alpha-Emitters.”)
In its attempt to disqualify the work of Cohen, the report also cites papers of Greenland and Morgenstern (1989); Smith et al. (1998); Stidley and Samet (1994); and the NAS/NRC BEIR VI (1999). Cohen thoroughly responded to all of these discussions of possible areas of discrepancy, as well as other arguments used against his work (Cohen 1988; 1994; 1997; 1998a; 1998b; 1998c; 2000a; 2000b; and Cohen and Colditz 1994). None of these papers is even mentioned in the NCRP report. In the case of Cohen and Colditz, the second author, Dr. Graham Colditz of Harvard University, is a most highly regarded epidemiologist. Dr. Colditz’s rigorous evaluation and analysis in this paper confirms that the analysis of Cohen’s data produces a highly significant negative correlation with radon levels, according to the highest standards of epidemiology practice. Yet, this paper is never addressed by those who claim that some undefined condition might cause an ecologic study to produce erroneous results. A statement in the NCRP report that the result of Cohen’s study “cannot be relied upon,” should perhaps end with the words “because it does not support LNT.”
Failing the Reality Test
It is sad and discouraging that NCRP-136 seeks to misrepresent the results of such a large number of sound and thorough studies, and fails to consider objectively the huge discrepancy between the observational data and LNT predictions, which clearly shows that LNT fails the test of reality. Treating many other studies in the same manner, it is our opinion that the NCRP committed a severe violation of the scientific method in defense of the obsolete LNT concept, which has now become a health and societal hazard.
References
Berrington, A., Darby, S.C., Weiss, H.A., and Doll, R., 2001. “100 years of observation on British radiologists: Mortality from cancer and other causes 1897-1997.” The British Journal of Radiology, Vol. 74, pp. 507-519.
Billen, D., 1990. “Spontaneous DNA damage and its significance for the ‘negligible dose’ controversy in radiation protection.” Radiation Research, Vol. 124, pp. 242-245.
Bogen, K.T., 1998. “Mechanistic model predicts a U-shaped relation of radon exposure to lung cancer risk reflected in combined occupational and U.S. residential data.” Human and Experimental Toxicology, Vol. 17, No. 12, pp. 691-696.
Calabrese, E.J. and Balwin, L.A., 2001. “Special Issue: Scientific Foundations of Hormesis.” Critical Reviews in Toxicology, Vol. 31, Nos. 4 & 5, pp. 347-695.
Calabrese, E.J., Balwin, L.A., and Holland, C.D., 1999. “Hormesis: a highly generalizable and reproducible phenomenon with important implications for risk assessment.” Risk Analysis, Vol. 19, pp. 261-281.
Cohen, B.L. 1988. “Dissociation between lung cancer and a geological outcrop.” Health Physics, Vol. 54, No. 2, pp. 224-225.
Cohen, B.L., 1994. “Invited Commentary: In defence of ecologic studies for testing a linear no-threshold theory.” American Journal of Epidemiology, Vol. 139, No. 8, pp. 765-768.
Cohen, B.L., 1995. “Test of the linear no-threshold theory of radiation carcinogenesis for inhaled radon decay products.” Health Physics, Vol. 68, No. 2, pp. 157-174.
Cohen, B.L., 1997. “Problems in the radon vs lung cancer test of the linear no-threshold theory and a procedure for resolving them.” Health Physics, Vol. 72, No. 4, pp. 623-628.
Cohen, B.L., 1998a. “The cancer risk from low-level radiation.” Radiation Research, Vol. 149 (May), pp. 525-528.
Cohen, B.L., 1998b. “Response to criticisms of Smith et al.” Health Physics, Vol. 75, No. 1, pp. 23-28.
Cohen, B.L., 1998c. “Response to Lubin’s proposed explanations of our discrepancy.” Health Physics, Vol. 75, No. 1, pp. 18-22.
Cohen, B.L., 2000a. “Explaining the lung cancer versus radon exposure data for USA counties.” Journal of Radiological Protection, Vol. 20, pp. 219-223.
Cohen, B.L., 2000b. “Testing a BEIR-VI suggestion for explaining the lung cancer vs. radon relationship for U.S. counties.” Health Physics, Vol. 78, No. 5, pp. 522-527.
Cohen, B.L. and Colditz, G.A., 1994. “Test of the linear no-threshold theory for lung cancer induced by exposure to radon.” Environmental Research, Vol. 64, pp. 65-89.
Doll, R., Sharp, C., Muirhead, C., and Darby, S., 1998. “Study of UK men who had participated in the UK nuclear weapons tests programme.” Journal of Radiological Protection, Vol. 18, No. 3, pp. 209-210.
Hohryakov, V.F. and Romanov, S.A., 1994. “Lung cancer in radiochemical industry workers.” Vol. 142, pp. 25-28.
Howe, G.R. and McLaughlin, J., 1995. “Breast cancer mortality between 1950 and 1987 after exposure to fractionated moderate-dose-rate ionizing radiation in the Canadian fluoroscopy cohort study and a comparison with breast cancer mortality in the atomic bomb survivors study.” Radiation Research, Vol. 145, pp. 694-707.
Jaworowski, Z., 1999. “Radiation risk and ethics.” Physics Today, Vol. 52, No. 9, pp. 24-29.
Kossenko, M.M. and Degteva, M.O., 1994. “Cancer mortality and radiation risk evaluation for the Techa River population.” The Science of the Total Environment, Vol. 142, pp. 73-89.
Kostyuchenko, V.A. and Krestinina, L.Y., 1994. “Long-term irradiation effects in the population evacuated from the East-Urals radioactive trace area.” The Science of the Total Enviroment, Vol. 142, pp. 119-125.
Littlefield, L.G., McFee, A.F., Salomaa, S.I., et al. 1996. “Do recorded doses overestimate true doses received by Chernobyl clean up workers? Results of cytogenic analyses of Estonian workers by fluorescence in situ hybridization.” Radiation Research, Vol. 150, pp. 237-249.
Liu, S.Z., Liu, W.H., and Sun, J.B., 1987. “Radiation hormesis: Its expression in the immune system.” Health Physics, Vol. 52, pp. 579-583.
Lubin, J.H., 1998. “On the discrepancy between epidemiologic studies in individuals of lung cancer and residential radon and Cohen’s ecologic regression.” Health Physics, Vol. 75, pp. 4-10.
Makinodan, T. and James, S.J., 1990. “T cell potentiation by low dose ionizing radiation: Possible mechanisms.” Health Physics, Vol. 59, pp. 29-34.
Matanoski, G.M., 1991. “Health Effects of Low-Level Radiation in Shipyard Workers,” The Johns Hopkins University, Department of Epidemiology, School of Hygiene and Public Health, Baltimore, Maryland 21205.
Miller, A.B., Howe, G.R., Sherman, G.J., Lindsay, J.P., Yaffe, M.J., Dinner, P.J., Risch, H.A., and Preston, D.L., 1989. “Mortality from breast cancer after irradiation during fluoroscopic examinations in patients being treated for tuberculosis.” The New England Journal of Medicine, Vol. 321, No. 19, pp. 1,285-1,289.
Moosa, M. and Mazzaferri, E.L., 1997. “Occult thyroid carcinoma.” The Cancer Journal, Vol. 10, No. 4 (July-August), pp. 180-188.
Moustacchi, E., 2000. “DNA repair: Consequences on dose-responses.” Mut. Res. Genet. Toxicol. Vol. 464, No. 1, pp. 35-40.
Muckerheide, J., Becker, K., Cihak, R., Cohen, B.L., Jaworowski, Z., Jovanovich, J., Kondo, S., Liu, Z., Luckey, T. D., Muckerheide, W.A., Patterson H.W., Pollycove, M., Rockwell, T., Seiler, F.A., Tschaeche, A., Walinder, G., and Wei, L., 1998. Low Level Radiation Health Effects: Compiling the Data. Radiation, Science & Health, Inc.
NCRP, 1954. Permissible dose from external sources of radiation. Washington, D.C.: U.S. Government Printing Office.
NCRP, 1975. Review of the current state of radiation protection philosophy. pp. 1-50. National Council on Radiation Protection and Measurements.
NCRP, 2001. Evaluation of the linear no-threshold dose-response model for ionizing radiation, pp. 1-287. National Council on Radiation Protection and Measurements.
Planel, H., Soleilhavoup, J.P., Tixador, R., Richoilley, G., Conter, A., Croute, F., Caratero, C., and Gaubin, Y., 1987. “Influence on cell proliferation of background radiation or exposure to very low, chronic gamma radiation.” Health Physics, Vol. 52, No. 5, pp. 571-578.
Robinette, C., Jablon, S., and Preston, T.L., 1985. “Studies of participants in nuclear tests.” Final Report. National Research Council.
Ron, E., Lubin, J., and Schneider, A.B., 1992. “Thyroid cancer incidence.” Nature, Vol. 360, p. 113.
Rossi, H.H. and Zaider, M., 1997. “Radiogenic lung cancer: The effects of low doses of low linear energy transfer (LET) radiation.” Radiation and Environmental Biophysics, Vol. 36, No. 2, pp. 85-88.
Shimizu, Y., Kato, H., Schull, W.J., and Hoel, D.G., 1992. “Studies of the mortality of A-bomb survivors. 9. Mortality, 1950-1985: Part 3. Noncancer mortality based on the revised doses (DS86).” Radiation Research, Vol. 130, pp. 249-266.
Smith, P.G. and Doll, R., 1981. “Mortality from cancer and all causes among British radiologists.” British Journal of Radiology, Vol. 54, pp. 187-194.
Stewart, R.D., 1999. “On the complexity of the DNA damages created by endogenous processes.” Radiation Research, Vol. 152, pp. 101-105.
Sutherland, B.M., Bennett, P.V., Sidorkina, O., and Laval, J., 2000. “Clustered DNA damages induced in isolated DNA and in human cells.” Proceedings of the National Academy of Sciences, Vol. 97, No. 1, pp. 103-108.
Suzuki, M., Nakano, K., Suzuki, K., et al., 1992. “Effect of chronic low dose irradiation of 60Co gamma rays in human embryo cells.” In Low Dose Irradiation and Biological Defence Mechanisms (T. Sugahara, L.A. Sagan, and T. Aoyama, eds.), pp. 307-310. Elsevier Science Publishers.
Tan, G.H. and Gharib, H., 1997. “Thyroid incidentalomas: Management approaches to nonpalpable nodules discovered incidentally on thyroid imaging.” Annals of Internal Medicine, Vol. 126, pp. 226-231.
Taylor, L.S., 1980. “Some non-scientific influences on radiation protection standards and practice.” Health Physics, Vol. 32, pp. 851-874.
Tokarskaya, Z.B., Okladnikova, N.D., Belayeva, Z.D., and Drozhko, E.G., 1997. “Multifactorial analysis of lung cancer dose-response relationship for workers at the Mayak Nuclear Enterprise.” Health Physics, Vol. 73, No. 6, pp. 899-905.
UNSCEAR, 1994. Sources and Effects of Ionizing Radiation. Report of the United Nations Scientific Committee on the Effects of Atomic Radiation. Annex B: Adaptive responses to radiation in cells and organisms. United Nations.
UNSCEAR, 2000. Sources and Effects of Ionizing Radiation. United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2000 Report to the General Assembly, with Scientific Annexes, pp. 1220. United Nations.
Walburg, Jr., H.E., 1975. “Radiation-induced life-shortening and premature aging.” Advances in Radiation Biology, Vol. 7, pp. 145-179.
Walinder, G., 1995. Has radiation protection become a health hazard? The Swedish Nuclear Training & Safety Center.
|
|
|
|
|
|
|
|